

Abstract
Background: WHIM (Warts, Hypogammaglobulinemia, Infections, Myelokathexis) Syndrome is a serious, ultrarare genetic disorder caused by a gain-of-function mutation in CXCR4 that causes profound neutropenia and lymphopenia associated with increased rates of bacterial and viral infections. Long-term sequelae include hearing loss, bronchiectasis, and HPV-associated malignancies. The cancer risk in WHIM patients is estimated at 30% by age 40. There is currently no treatment that addresses the underlying mechanism of disease. G-CSF increases neutrophil counts but does not appear to reduce infection rates; use of parenteral gamma globulin has had mixed reports of benefit, but no controlled trials have been reported; Plerixafor, a CXCR4 antagonist, has been shown to increase leukocyte counts and reduce infection rates when absolute neutrophil counts (ANC)>600 mm-3 and absolute lymphocyte counts (ALC)>1000 mm-3, but is a parenteral agent that must be administered twice daily. X4P-001 is an orally available, allosteric inhibitor of CXCR4 that is being developed to treat WHIM. We report here the PK/PD data from the Phase 2 portion of Phase 2/3 trial X4P-001 MKKA (NCT03005327) in WHIM patients that led to selection of the dose for Phase 3 development.
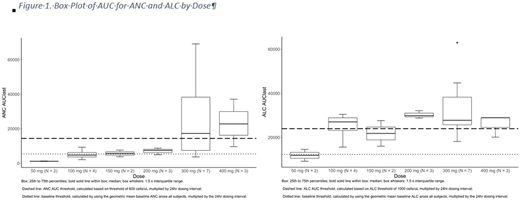
Methods: Study X4P-001 MKKA is a Phase 2/3 study. The primary objective of Ph2 portion was to assess the dose required to achieve a consistent increase in circulating neutrophils and lymphocytes. Adult patients with WHIM syndrome, with documented WHIM-associated genotype, and either ANC <400 mm-3 and/or ALC<650 mm-3 were treated with escalating doses of X4P-001. After at least 5 weeks on a dose, patients were hospitalized overnight for rich PK sampling. At each sampling point ANC and ALC were also determined. An area under the curve for ANC and ALC was calculated using the trapezoidal rule and normalized to AUCs assuming maintenance of the threshold values of 600 mm-3 for ANC and 1000 mm-3 for ALC over 24hr. Dose escalation was permitted for adjusted AUC value <0 cell/hours/μL. AUC values ≥0 were considered as having met the primary objective for Phase 2.
Results: Eight patients were enrolled and were evaluable for efficacy. 6 of 8 were female, and the mean (SD) age was 35.5 (13.37). Two patients started treatment with 50 mg, then received, 100, 150, 300 and 400 mg; 2 started at 100 and then received 200 and 300 mg; 2 started at 200 mg; 1 escalated to 300 and 400 mg while the other terminated after 1 week due to an adverse event (AE). Two started at 300 mg and did not escalate. Doses of at least 300 mg/day were needed to achieve success criteria for ANC, while at doses ≥100 mg/day, 50-100% met success criteria for ALC. (Figure 1)
Two patients discontinued: 1 due to an AE of grade 1 rash, and 1 voluntarily withdrew. No serious AEs were reported. One patient had unrelated cholecystitis (grade 3). All other AEs were grade 1 or 2.
Conclusions: Treatment of WHIM patients with X4P-001 results in meaningful increases in ANC at doses ≥300 mg, and in ALC at doses ≥100 mg per day for at least 5 weeks. These doses are anticipated to be associated with clinically meaningful outcomes in terms of infections and warts. X4P-001 appeared to be safe and well-tolerated at doses of 50-400 mg per day.4
Dale:Athelas, Inc.: Equity Ownership; Amgen: Consultancy, Research Funding; Sanofi-Aventi: Consultancy, Honoraria; Cellerant: Other: Scientific Advisory Board; Hospira: Consultancy; Prolong: Consultancy; Beheringer-Ingelheim: Consultancy; Coherus: Consultancy. Hartmann:Cetara: Employment; X4P Pharmaceuticals: Consultancy. Brown:Certara: Employment; X4P Pharmaceuticals: Consultancy. Ebrahim:X4Pharmaceuticals: Employment. Gorelick:X4 Pharma: Consultancy; PIN Pharma: Consultancy; Shire: Consultancy; NGN Capital: Consultancy, Other: Venture partner; IntraBio: Consultancy; Zymo Consulting Group LLC: Employment.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal